This condition is also known as:
- Chronic (histiocytic) intervillositis of unknown etiology (CIUE)
- Massive Chronic Intervillositis (MCI)
- Nonspecific Chronic Macrophagic Intervillositis
- Histiocytic Intervillositis (HI)
Similar conditions include:
- Chronic Villitis
- Chronic Villitis of unknown etiology (CVUE)
Related conditions include:
- Massive Perivillous Fibrin Deposition (MPFD)
- Villitis of Unknown Etiology (VUE)
When it was first mentioned:
First specific description in the literature by Labarrere and Mullen in 1987 in the American Journal of Reproductive Immunology “Fibrinoid and Trophoblastic Necrosis with Massive Chronic Intervillositis: An Extreme Variation of Villitis of Unknown Etiology“
Clinical Definition*:
- Idiopathic inflammatory lesion
- Intervillous space location
- Extensive maternal infiltration of inflammatory mononuclear cells (monocytes, lymphocytes, histiocytes) in particular CD68
- Intervillous fibrinoid deposits and trophoblast erosions of varying degree
- Diffus (massive) or multifocal infiltration
- CHI is considered to be CIUE when accompanied by no other evidence of either villosistis or other placental lesion.
Clinical Information*
- Pregnancy loss at any gestation age, most common in first trimester
- Poor outcome: (severe) IUGR (Intrauterine growth restriction or Intrauterine Growth Retardation), IUFD (Intrauterine Fetal Demise), stillbirth, spontaneous abortion/miscarriage
- Perinatal mortality 29%, IUGR 77%**
- Recurrence rate between 30-90% (depending on studies)
- Normal karyotype
Incidence (how common is it?)
- Considered a rare placental inflammatory disease
- Currently diagnosed in approximately 1% of spontaneous abortions/miscarriages and
- in less than 1% of placentas in 2nd and 3rd trimester*
- frequently missed diagnosis with a high recurrence risk
This is a cause of concern because of the severe issues linked with the diagnosis, it is possible that is it more common than we realise in cases of recurrent miscarriage for example as placentas may not always be analysed after an event. The same for cases of IUGR with live birth outcome. Furthermore from some research that I have performed I continue to see cases of CHI being exhibited to Pathologists in conferences so Pathologists themselves are still being educated on how to recognise it when analysing the placenta. If they don’t know what they are looking for they won’t spot it and it won’t be diagnosed.
What Causes It?
At this current time the trigger is unknown, possible immunologic origin, most likely alloimmune due to the nature. CHI might also be confused with infectious placental lesions observed in; malaria, listeriosis, tularemia, CMV, herpes etc. Polymorphous inflammatory infiltrate.
“CHI – An immune Reaction to the Baby or Immunity to Pregnancy
Women with this problem make antibodies to DNA components in the embryo, or in the pregnancy tissue that surrounds it. These antibodies form first in the blood and later graduate to the lymphatic system and the tissue. After repeated losses, antibodies to DNA components can develop into antibodies that occupy organs such as the uterus, and cause local inflammation that may contribute to further miscarriage. For CHI sufferers this manifestation of where antibodies to the baby and components of placental DNA cause inflammation in the placenta. These (are) Category 3 problems (which) are graded “severe”, “moderate”, or “mild”.
a). Villitis
Villitis is inflammation in the tissue of the root system of the placenta known as the villus. The inside of the villus contains the blood vessels of the placenta that will eventually join the larger vessels in the umbilical cord. Antibodies to DNA can cause inflammation of the entire villus.
b). Intervillositis
When the inflammation is severe and spreads from one villus root to another and there is inflammation between them.
c). Decidual inflammation
The inflammation can also spread into the decidua to which the placenta is attached.”
What Dr. Beer says (Pg 12, 61, 137 of Is Your Body Baby Friendly?)
(Disclaimer: Whilst sections from this publication are included NK cell investigation in relation to CHI is not endorsed as a logical treatment plan by the author of this paper)
What Happens in Laymans terms?
The immune system launches an attack on the placenta which then gets clogged up by histiocyte cell ‘junk’ that the mother fires into the intervillous space (the space in between the finger-like vessels of the placenta). Normally the baby will not know this is happening unless the problem is untreated for four weeks. In a normally functioning placenta, the space should be full of free flowing nutrient-rich blood, which then flows to baby after an ‘attack’ it becomes a car park of histiocytic junk. To understand where all these bits are please have a look at the following diagrams:
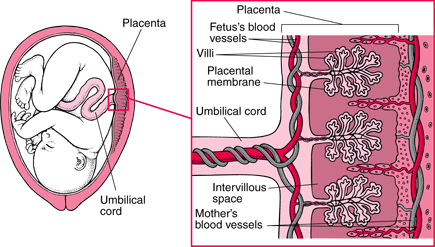
Courtesy of Michael R. Foley, M.D. (2007) http://www.merck.com/mmhe/sec22/ch259/ch259a.html
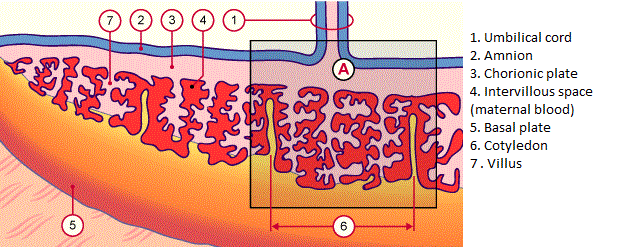
Diagram courtesy of http://www.embryology.ch/anglais/fplacenta/villosite01.htm
What does this mean?
If the attack goes untreated it results in insufficient blood flow to the baby, hence reverse Dopplers or Reverse End Diastolic flow. Reverse flow normal indicates the need for immediate delivery, leaving a baby in the womb with this finding means the baby is conserving all the blood it does receive and trying to direct it to vital organs, in a bid to survive. Everything is sent to the brain and heart, but this is unlikely to be enough and is sure to result in brain and heart damage. This is also why the fluid levels drop, (often expressed as Oligohydramnios or Anhydramnios) as the baby stops urinating.
Symptoms:
In Pregnancies less than 12 weeks
- Spontaneous miscarriage before 12 weeks
- High white blood cell count and/or Neutrophils, Monocytes (to be confirmed, a number of ladies have reported this)
In pregnancies 12+ weeks
- Restricted growth (severe) IUGR of an otherwise chromosomal normal foetus
- Reduced amniotic fluid
- Early warning of IUGR is a marked slowed down in growth or long bones (such as femur) on growth scans
- Abnormal dopplers showing indicating redistribution, intermittent absent flow and then eventually reverse end diagnosic flow.
How can we check this diagnosis?
At this time the only way to check for this diagnosis is to have a Post Mortem where the placenta is analysed by a pathologist who will cite CHI through checking the placenta.
Ask your Pathologist to perform CD68 Immunostaining to check the levels of this particular cell. Sufferers will have elevated numbers of these cells in the placenta.
Next Steps
CHI pregnancies that end in a loss are very traumatic. A high number of women diagnosed after a pregnancy loss go on to exhibit one or more signs of PTSD. Even if later you have a successful birth you can experience anxiety or a number of other mental health conditions that are directly connected to the particular prolonged and stressful situation that CHI puts you in. It also may have negative implications for partnerships and on partners involved. Before trying again it is highly recommended and extremely important for your wellbeing that you seek professional guidance or counselling, either through your healthcare professional your local child bereavement charity who may be able to put you in contact.
Finally, when you are ready, connect with a CHI Specialist at one of our Centres of Excellence (the list is available from the home page) either directly or through your trusted healthcare consultant. Together they can work together to advise the best course of action in any future pregnancies you may have.
Other Reading
Summary of suggested treatments for Chronic Histiocytic Intervillositis (CHI)
Sources:
- Am J Reprod ImmunolMicrobiol. 1987;15:85:91. Fribrinoid and trophoblastic
necrosis with massive chronic intervillitis: An extreme variant of villitis of
unknown etiology. Labarrere CA, Mullen E. - Pediatric and Development Pathology. 2006;9:234-8. Co-occurance of Massive
Perivillous Fibrin Deposition and Chronic Intervillositis: Case Report. Weber MA,
Nikkels PGJ et al. - Gynecol Obstet Biol Reprod (Paris). 2006;35(7):711-9. Pronostic périnatal des grossesses compliquées d’intervillites chroniques placentaires: C. Rota, D. Carles, V. Schaeffer, F. Guyon, R. Saura, J. Horovitz Rota C. et al.
- Placenta. 2010;31:1106-10. Chronic intervillitis of the placenta: A systemic review. Contro E. et al.
- Placenta. 2010;31:116-9. Pathological charactéristic of a series of rare chronic
hystiocytic intervillisitis of the placenta. Traeder J. et al. - Chronic histiocytic intervillositis of unknown etiology: Clinical features in a consecutive series of 69 cases: Marchaudon et. al
- Massive perivillous fibrin deposition and chronic intervillositis: frequently missed diagnoses with a high recurrence risk: MA Weber, PGJ Nikkels, KE Hamoen, JJ Duvekot, RR de Krijger
- Arch Pathol Lab Med. 2012;136:657–659; doi: 10.5858/arpa.2011-0328-OA CD68 Immunostaining in the Evaluation of Chronic Histiocytic Intervillositis Debra S Heller MD
*No date attached to this percentage
** Source does not quote where these figures are from check Boog et al. J Gynecol Obstet Biol Reprod (Paris). 2006 Jun;35(4):396-404. [Association des corticoïdes à l’aspirine pour la prévention des récidives de villite ou d’intervillite chroniques d’étiologie indéterminée: G. Boog, C. Le Vaillant, F. Alnoukari, F. Jossic, J. Barrier, J.-Y. Muller ]